
SGLT-2 Inhibitors including Invokana (canagliflozin), Farxiga (dapagliflozin), Jardiance (empagliflozin) and Steglatro (ertugliflizin), are the newest class of oral medications for the treatment of type 2 diabetes. In order to understand how these medications work, let’s start by looking at how the kidney handles glucose.
It Starts with the Kidneys
Your kidney works by filtering all of your blood and sorting out which nutrients or electrolytes your body wants to keep and which should be excreted into the urine. When the blood sugar is normal, your body reabsorbs all of the glucose so it can go back into the blood to be used for energy rather than excreted in the urine. When your blood glucose gets too high (over ~200 md/dL), the kidney will dump some of the glucose in the urine since your body does not need all of the excess glucose. SGLT-2 inhibitors block your kidney’s ability to reabsorb glucose. This means that more glucose will be excreted into the urine and less sugar will be reabsorbed back into the blood thereby lowering the blood glucose and A1C levels over time. In addition, when you urinate out excess glucose or sugar you will have the tendency to lose some weight. In more simple terms, SGLT-2 inhibitors work by making you pee out your excess glucose so your A1c gets better and you lose weight.
When this happens, you may also urinate slightly more water than usual as well. This is also the reason why some, but not all, people say that they are more thirsty and urinate more frequently than normal. These symptoms affect a small minority of people while using these medications, primarily when you start the medication, and then the symptoms subside over time.
Pros and Cons
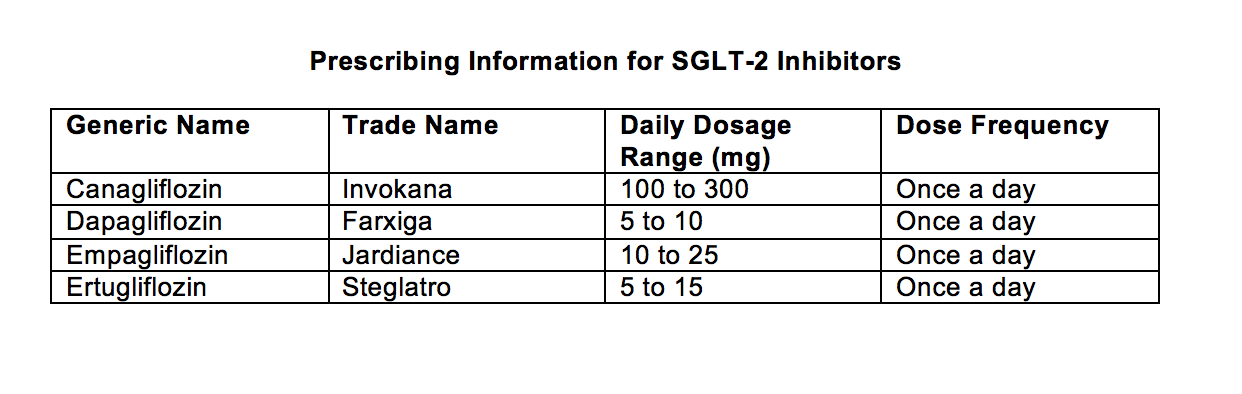
Invokana, Farxiga, Jardiance and Steglatro are effective once-daily oral medications which are generally very well tolerated. They are associated with weight loss compared with other oral medications to treat type 2 diabetes which are either weight-neutral or have no effect on weight (such as metformin and DPP4-inhibitors) or cause weight gain (such as SFUs and TZDs.) In the recent EMPA-REG Cardiovascular Outcome trial, Jardiance was found to decrease passing away from cardiovascular disease in people with diabetes who were already at risk for heart problems and decreased the progression of diabetic kidney disease. Similar results were seen in the Cardiovasculars Outcome trial with Invokana and Farxiga. The study to evaluate the heart safety effects of Steglatro has not been completed yet, but the benefits on the heart are expected to be seen in all four. (More info on preventing heart attacks and preserving the life of your diabetic kidney can be found in chapters 12 & 13 in my Taking Control of Your Diabetes book). Since these medications rely on good kidney function in order to work, they cannot be used in patients with moderate to severe kidney dysfunction or in patients on dialysis. See the table below for the prescribing guidelines.
 Lastly, there is a new SGLT inhibitor currently being developed by Lexicon and Sanofi. If approved, Zynquista (sotagliflozin) will be indicated for people with type 1 diabetes.
Lastly, there is a new SGLT inhibitor currently being developed by Lexicon and Sanofi. If approved, Zynquista (sotagliflozin) will be indicated for people with type 1 diabetes.
Potential Side Effects
SGLT-2 inhibitors can cause a decrease in blood pressure which can be good for many patients, but for others who may be elderly or on potent diuretics (water pills), it can cause hypotension (blood pressure gets too low). Other potential side effects also include dehydration so you should discuss this with your doctor if you are already taking diuretics. SGLT-2 inhibitors can also cause genital yeast infections, especially in women and uncircumcised men. This problem occurs in a minority of people but it is important to be on the lookout for it. Another very rare complication seen with SGLT-2 inhibitors is a problem called “euglycemic diabetic ketoacidosis” (DKA). DKA is usually a complication of type 1 diabetes when insulin levels are too low (from skipped insulin doses, etc.) but it can occur in patients with type 2 diabetes as well.
Looking Out for DKA
Normally DKA is associated with very high blood sugar levels. However, when it occurs from taking an SGLT-2 inhibitor, DKA can happen with relatively normal blood sugar levels. Symptoms of DKA include profound fatigue, nausea, vomiting, abdominal pain, or a fruity odor on the breath regardless of the blood glucose level. If you are taking an SGLT-2 inhibitor, you should watch for these symptoms and report them immediately to your HCP if they occur. Many health care professionals are prescribing ketone meters to their patients who may be at risk for DKA.
DKA is a very uncommon and easily treated condition but nonetheless a level of awareness is important. If anyone develops any symptoms of DKA, they should stop the medication, test glucose and ketone levels, drink fluids and take insulin and carbohydrates. Carbohydrates are important since they turn off the body’s drive to produce ketones, which are the culprits causing DKA with these medications.


Dr. E,
I have ckd stage 3 and for the past few years the creatinine levels have fluctuated between 1.6 to 1.8 but staying pretty much stable at that. Started seeing a nephrologist and she decided to make some changes to diabetes meds and put me on Jardiance 10 mg. I have been on that for about 3 months. I just did labs and my creatinine levels are now 2.0. I think Jardiance is a problem after reading about it. I know you can’t say much without seeing all the labs, but do you have an opinion with this much info?
Thanks, Paula
If you have Stage 3 CKD, then I would take Jardiance. Make sure you are hydrated and test again with an eGFR, and make sure you get your microalbumin to creatinine ratio as well.