
Meet the Patient: Natalie
Natalie is a 47-year-old Caucasian woman who has had type 2 diabetes for 10 years.
Like many people with type 2 diabetes, she also has central obesity (a.k.a. belly fat), high blood pressure, and elevated triglycerides. Triglycerides are a type of fat in your blood that, when too high, can increase your risk of heart disease.
When Natalie was first diagnosed with diabetes, her doctor started her on the following meds:
- Metformin to manage blood glucose
- An ACE inhibitor for high blood pressure
- Gemfibrozil to address high triglycerides
Her A1c was consistently around 8.8% – not great.
In 2018, her doctor added Ozempic to her regimen to help improve her blood sugars and help her lose weight.
Natalie doesn’t wear a CGM, but she does check her blood sugars the old fashioned way with fingersticks.
DKA and SGLT2 Inhibitors: An Unexpected Side Effect for Natalie
A few months ago, Natalie’s routine labs revealed something her doctor had been watching closely – her kidneys were starting to show signs of trouble. To help protect her kidney and heart health – and to give her blood sugars an extra nudge – her doctor prescribed an SGLT2 inhibitor.

SGLT2 medications not only support kidney and heart health, but they also help lower blood sugar by encouraging the kidneys to flush out extra sugar through the urine. (Come on kidneys, you can do it! Pee out that glucose!)
A few weeks after starting the medication, Natalie started feeling off. At first it felt like she had the flu – headaches, body aches, fatigue, and dry mouth. Her blood sugars were high but not alarmingly so – just in the low 200s mg/dL.
She decided to rest and ride it out, but things didn’t improve. Soon, nausea and vomiting hit her hard, and she couldn’t keep anything down. Her husband rushed her to the ER, where doctors admitted her to the ICU with something more serious than the flu – DKA.
DKA and Type 2 Diabetes: More Common Than You’d Think

DKA is a serious medical condition that happens when your body doesn’t have enough insulin to move sugar into your cells for energy. Without enough insulin, your cells can’t get the sugar they need, so you start burning fat for fuel instead. This process leads to ketone production, and a high level of ketones leads to DKA.
DKA is more common in people with type 1 diabetes, but people with type 2 diabetes who are under poor control and/or on SGLT2 inhibitors can develop it too. If left untreated, DKA can be life-threatening.
Common symptoms of DKA include headache, muscle aches, fatigue, extreme thirst, dry mouth, frequent urination, difficulty breathing, fruity-smelling breath, stomach pain, nausea, and vomiting.
Euglycemic DKA: A Lesser-Known Form of DKA
One of the classic red flags for DKA is super-high blood sugar – we’re talking in the 400–500 mg/dL range – but there’s a fairly common variant called euglycemic DKA when your blood sugar isn’t super high – levels could even be below 200 mg/dL!
There are a few different reasons for euglycemic DKA, and one of them is due to the effects of SGLT2 medications. As we mentioned earlier, SGLT2s lower blood sugar by helping your kidneys flush out extra sugar through your urine. With less sugar in your blood, your body may produce less insulin, and that shift can sometimes set the stage for euglycemic DKA. This is why euglycemic DKA can be more common in people with type 2 diabetes.
Natalie’s doctor didn’t warn her that this could happen with SGLT2 medications, but unfortunately that’s all too common. People with type 2 diabetes often don’t know about DKA because their doctors don’t cover it.
The Solution: How to Treat DKA in Type 2 Diabetes
If you’re on an SGLT2 inhibitor, the first step in treating DKA is to stop taking it. If you’re able to hold down food and liquids and you have insulin at home, you should take a rage bolus of insulin (the recommendation is 1.5 times your normal insulin dose, but everyone’s needs will be different), consume 30 to 60 grams of carbs, and drink lots of fluids.
If you aren’t on insulin, stop your SGLT2 medication and start drinking fluids. If your blood sugar is not through the roof (below 200 mg/dL) consume 30-60 grams of carbs too. If you have high blood sugar, just drink fluids.
Regardless of whether or not you are on insulin, if you can’t hold down food or liquids, you need to go to the hospital to be treated.
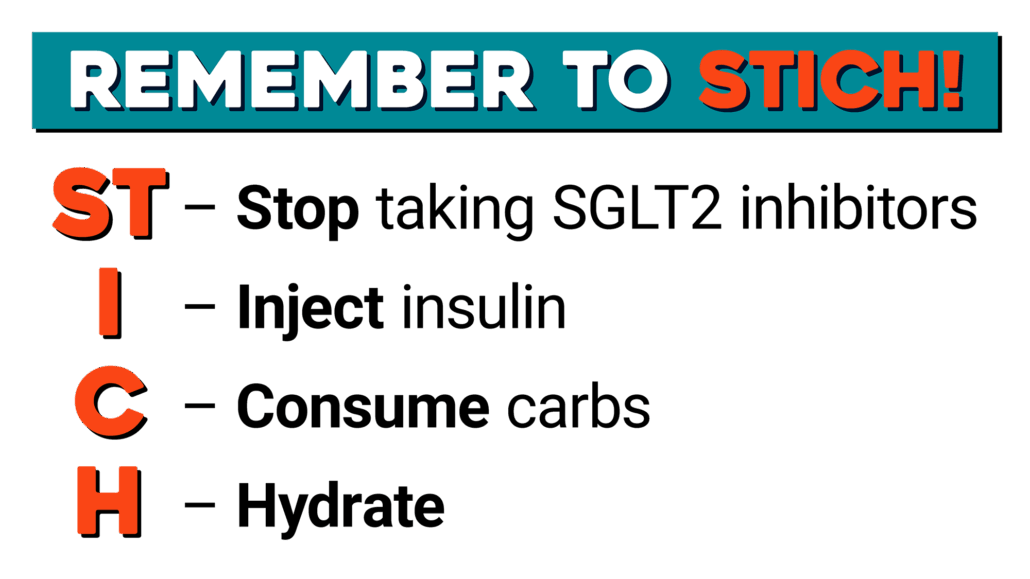
A simple way to keep DKA treatment steps straight is by using the STICH protocol:
- STop taking SGLT2 inhibitors.
- Insulin: Take a rage bolus of insulin.
- Carbs: Ingest 30 to 60 grams of fast-acting carbs.
- Hydrate: Drink low-calorie liquids like water or zero-sugar sports drinks to help flush the ketones out. Regular Gatorade can work in this case as both a fluid and a carb source.
What’s Next for Natalie?
Natalie was in the ICU for a few days. She was discharged once her DKA was treated and it was no longer an issue.
After her hospital stay, Natalie’s doctor started her on basal insulin to help bring her A1c down. A lower A1c will reduce her risk of DKA in a big way. As soon as she went on insulin, her insurance covered a continuous glucose monitor (CGM), giving her better insight on her day-to-day blood sugars.
When it comes to restarting her SGLT2 medication, that’s a decision Natalie and her doctor will need to revisit together. These meds can provide powerful heart and kidney benefits, and for many people the risks are quite low (one study showed a .2% risk) but it’s important to weigh the benefits against potential risks for each individual.
When continuous ketone monitoring becomes available (possibly within the next six months!) Natalie would be an ideal candidate because she’d be notified right away if her ketones started to creep up.
DKA and Type 2 Diabetes: Key Takeaways
The connection between DKA and SGLT2 inhibitors means people can develop diabetic ketoacidosis even when their blood sugar levels are not severely elevated.
On paper, Natalie didn’t check the typical boxes for DKA risk. Her DKA wasn’t due to insufficient insulin because she wasn’t taking any, and she wasn’t battling the flu or a nasty infection. However, her diabetes control was poor, and that put her at a higher risk. The higher your A1c, the higher your risk for DKA. Those who are most at risk have an A1c close to 9% or higher.
The good news? If your type 2 diabetes is well controlled, your risk of DKA is very low.
But everyone who’s on insulin or an SGLT2 inhibitor – including all people with type 1 diabetes – should know the warning signs of DKA, and have a blood ketone meter with unexpired test strips on hand just in case.
DKA is serious, and unfortunately not uncommon. Awareness and recognition are the keys to prevention and early management of the condition.
Explore our resource library and video vault, and subscribe to our monthly digital newsletter for more tips, tools, and expert guidance on how to take control of your diabetes.

I hope Natalie’s providers consider that she might have LADA even without a positive antibody test.
You’re right…not many people know about autoantibody-negative type 1 diabetes. Thanks for the commment!
Dear Doctors and readers,
I’m planning a trip to Japan leaving Thursday 12:00 a.m. Arriving Tokyo Friday AT 5Pm. Then leaving Tokyo Tuesday and arriving Los Angeles at 5PM Tuesday.
So that means I will not have dialysis Friday and Monday. I know I’m healthy but am I taking a risk. Off dialysis for 2 days?
Thanks for your opinion.
Arlene N.
You should discuss this with your nephrologist.
https://www.kidney.org/kidney-topics/missing-dialysis-treatment-dangerous-your-health
I would love to answer that question for you, but I would definitely ask your kidney doctor.