The Patient:
Harry is a 77-year-old male physician with a long history of type 2 diabetes and chronic kidney disease (stage 3b) among other medical problems. His eGFR is 25-30 and his urine albumin to creatinine ratio (UA/Cr) is over 300 mg/g, which indicates chronic kidney disease. He is on two medications that protect his kidneys – Kerendia and Farxiga – and he’s being seen by a nephrologist. He also takes Trulicity for his diabetes.
Harry’s 30-day FreeStyle LibreView Download Data:
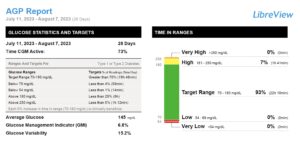
As you can see from the download, Harry’s time in range is excellent – above 90% (goal above 70%) and without hypoglycemia! His glucose variability is less than 20% (goal less than 37%). His estimated A1c (referred to in the report as GMI or glucose management indicator) is 6.8%.
The Problem:
When I ordered Harry’s laboratory work, his A1c came back at 4.9%, which is much lower than you’d expect for the blood sugars that are documented on his CGM report.
It’s well known that chronic kidney disease and anemia (which goes along with CKD) can give someone a falsely low A1c. This is why time in range and another CGM metric such as GMI (or estimated A1c) are so important, because those glucose levels are not affected by chronic kidney disease as the A1c is.
There’s a whole list of other medical conditions that can give inaccurate A1c levels, such as pregnancy, sickle cell trait, liver disease, and being part of certain ethnic groups. See the list below for the many conditions that can affect an A1c result:
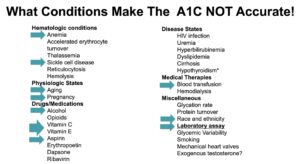
How Laboratory Blood Work Is Affected by CKD
People with CKD are anemic. The A1c measures glucose bound to red blood cells, and if you’re anemic you don’t have many red blood cells so you’re measuring the glucose bound to a fewer number of red blood cells. Anything that causes anemia will cause a falsely low A1c, which can be very misleading and lead to inappropriate insulin management decisions. A lot of doctors, quite frankly, miss it. Harry’s low A1c would fool many doctors who aren’t knowledgeable about the relationship between chronic kidney disease and the accuracy of the A1c test.
The Takeaway:
People with CKD or any condition that causes anemia need to know that their A1c may not be accurate. It’s not uncommon for people with poor glucose control (like an estimated A1c of 8.5 or higher on their CGM) to get a lab A1c result of 6.9 and then their doctor pats them on the back and tells them they’re doing great. The A1c used to be all we had to judge long-term diabetes control, but the availability of CGM devices and the metrics they can provide really uncover the pitfalls of the A1c test.
My patient Harry is actually doing really well diabetes-wise, based on his CGM. There are a lot of reasons why an A1c may be inaccurate, and that’s why time in range and estimated A1c or GMI from a CGM are much better indicators of long-term glycemic control.
Additional Resources:
Why the A1c Sucks (and Why Time in Range Is More Important)
A Dose of Dr. E: Why the A1c Sucks
Which Is Better…a Lab A1c Test or the Estimated A1c (GMI) from a CGM?
CKD: Diabetes Can Put You at Risk for This Silent Disease
Live Long and Prosper with Kerendia, a New Medication for Type 2 Diabetes

I really enjoy hearing your information. I always learn something. Thank you so much.
Thanks Donna – appreciate it!
I have CLL, leukemia which causes low red blood count. It’s taken me along time for me to convince my care providers that A1c is useless for me. I do very well with my cgm. I use the time in tight range. Thank God for cgm. Most of my Doctors including my Retinal doctor barely know what a CGM is nor do they know what to do with the information I provide them. They all just want to know what my morning number was that day. The number is useless because I manipulate the number if my cgm wakes me up in the middle of the and tells me it’s going high or low. It’s also hard for them to understand the charts my cgm generate because I go to bed around 3AM and wake up around 11AM. I’m on Mounjaro and don’t have any desire to eat a breakfast so the doctors don’t understand why there is no raise in my blood sugar levels until late in the day. Oops, it’s 12:35 AM and my smart watch, my phone and my Sugar Pixel say I’m heading for a low, so I’ll go eat something. Good evening.
You are right in that the A1c is not very valuable, and hopefully with time, doctors will get more familiar with CGM.
What about Fluoride dental treatments influencing glucose levels…I think this is another hidden factor in managing A1c and glucose levels in general.
See: https://fluoridealert.org/studies/diabetes02/
Thanks so much for the information. Appreciate it.
So, a test for anemia should be done along with testing A1c?
What about Fluoride dental treatments influencing glucose levels…I think this is another hidden factor in managing A1c and glucose levels in general.
See: https://fluoridealert.org/studies/diabetes02/
Thanks to you for TCOYD, and all you do to help make living with T1D easier.
No. Your PCP should be ordering tests once or twice a year that cover your general health and things like anemia…such as the CBC.