
What are Hybrid Closed Loop Insulin Pump Systems?
Hybrid closed-loop systems are incredible technology, but they can’t go it alone (at least not yet). “Hybrid” means that you still have to interact with your pump to enter carbs or mealtime boluses.
A fully closed-loop system (which is not commercially available yet) means you never have to interact with your system or enter carbs. You just go through life eating anything you want, and the system adapts. The iLet is about the closest you can get to a fully closed-loop system, but you still have to announce meals.
Hybrid closed-loop systems do a lot of the heavy lifting, but they still need you to give them direction.
Many providers start new pump users out with conservative settings. If those settings aren’t adjusted over time, they can end up holding you back from achieving the best possible glucose control.
Target Glucose Level: Your Blood Sugar Bull’s Eye

Your target glucose level is the number your algorithm is constantly working to keep your blood sugar levels close to 24/7. Some systems allow you to choose an exact number, while others have a target range.
When your blood sugar goes above target, the system increases insulin delivery to bring you back down. If you dip below target, it eases up and even stops insulin delivery to prevent an impending low. Every automated adjustment is guided by this one setting. Each system has its own adjustable targets.
How to Maximize Your Target Glucose Level
Choose the lowest target (or target range) allowable with your system. If your system is shooting for a lower target, you’re going to have better glucose control. However, the goal is to have the best time in range for your individual needs with the least amount of hypoglycemia. If you start having too many lows, you may need to look at your other settings and/or potentially raise your target glucose, at least temporarily.
Insulin-to-Carbohydrate Ratio (ICR): How Much Insulin You Need When You Eat

This is a very important individualized bolus setting.
Before we get into the nitty-gritty, know that everyone has problems trying to figure out how much insulin to take with meals – even if you’ve lived with diabetes for 50 years!
The insulin-to-carb ratio determines what your glucose will be 1-2 hours after eating. A good goal for most people is between 50-100 mg/dLs above the level you were at when you started your meal. Of course, it all depends on what you eat – a heavy carb meal is going to be different from a heavy protein meal, so you have to experiment.
Keep in mind, you can’t really judge your insulin-to-carbohydrate ratio if you take your insulin right when you eat – you have to take your insulin 15-30 minutes ahead of the meal, depending on your blood sugar (the higher your blood sugar, the earlier you should take your insulin before eating).
The insulin-to-carbohydrate ratio calculation determines how much insulin you need to cover the carbs you eat.
A common starting formula healthcare providers use is called the 500 rule:
500 ÷ your total daily insulin dose (TDD)
For example:
If you use 50 total units per day (basal + bolus), 500 ÷ 50 = 10. That gives you an ICR of 1:10, meaning you need 1 unit of rapid-acting insulin for every 10 grams of carbs.
This formula is often used when someone is newly diagnosed, and for many people, it underestimates how much insulin they actually need for meals.
A more aggressive strategy uses this formula:
350 ÷ your total daily dose
For example:
If you use 50 total units per day, 350 ÷ 50 = 7. That gives you an ICR of 1:7, meaning you need 1 unit of rapid-acting insulin for every 7 grams of carbs. You get more insulin before you eat, with the idea that your post-meal blood sugars will improve.
How to Maximize Your Insulin-to-Carb Ratio
If your post-meal glucose spikes regularly go up over 100 mg/dL from where you started before the meal, try using the more aggressive ICR formula and divide 350 by your total daily dose.
Correction Factor (CF): How Much Insulin You Need to Bring Down a High

The correction factor (also called the insulin sensitivity factor, or ISF) is how much 1 unit of insulin will lower your glucose (assuming it is level with a horizontal trend arrow). It tells your system how to correct a high blood sugar.
A common starting formula for newbies is:
1800 ÷ your total daily insulin dose
For example:
If you use 50 total units per day, 1800 ÷ 50 = 36. That means 1 unit of insulin is expected to lower your glucose by about 36 mg/dL. So if you’re 72 mg/dL above your target, your system would calculate 2 units for correction.
Like the 500 rule for carb ratios, this formula is intentionally conservative and often underestimates how much insulin is actually needed.
A more aggressive approach uses this formula to determine the correction factor for insulin:
1500 ÷ your total daily dose
Using the same example, 1500 ÷ 50 = 30. This means 1 unit of insulin lowers glucose by about 30 mg/dL instead of 36 mg/dL, so your system delivers more insulin when correcting highs.
When and How to Maximize Your Correction Factor
When your blood sugar is elevated (e.g., 220 mg/dL with a trend arrow straight across), how much insulin do you need to bring your glucose down to your target range? If your glucose doesn’t come down in 1-3 hours, or doesn’t get there at all, then using the more aggressive correction factor formula of dividing 1500 by your TDD will help.
Duration of Insulin Action (DIA): How Long Insulin Works In Your Body After It’s Delivered
The duration of insulin action (also called “active insulin time” or AIT) is the amount of time insulin stays active in your body. It tells the bolus calculator how long insulin will remain active after a bolus. It also helps calculate the remaining insulin on board from previous manual or correction boluses.
A longer DIA (4-5 hours) makes the algorithm more conservative because it thinks the insulin is actively working in your body for that amount of time. This can mean slower corrections and more time running high.
With a shorter DIA (2–3 hours), the system assumes insulin’s effect fades faster, so it can respond more aggressively to rising glucose levels. This can help improve time in range.
How to Maximize Your Duration of Insulin Action
Not all pumps allow you to adjust this setting, but if yours does, setting it as short as possible (2 hours is often recommended) will allow the system to be more aggressive.
Basal Rate: The Behind-the-Scenes Backbone of HCL Systems
Even though hybrid closed-loop insulin pump systems adjust basal delivery dynamically, your programmed basal rate is still important.
If your basal is too low, you may see prolonged hyperglycemia overnight (or in between widely spaced meals).
If your basal is too high, the system repeatedly suspends insulin, and you risk rebound highs.
A good basal profile means glucose stays stable when you’re fasting, with minimal correction needed overnight. Remember that these hybrid closed-loop systems are very sophisticated, and when one setting is off, the others compensate. They all work together to keep glucose at the target range.
How to Maximize Your Basal Rate
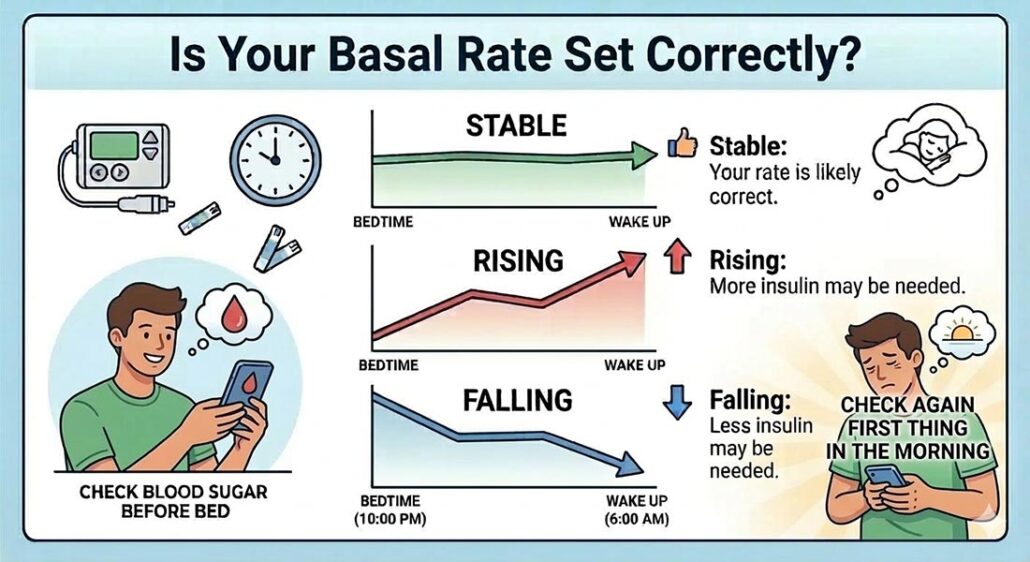
Your basal rate is working correctly when it keeps your blood sugar stable overnight (or between long periods of fasting).
Here’s how to test it: Check your blood sugar before bed and again first thing in the morning – if it stays relatively flat overnight, you’re likely in good shape. You can run the same test between meals. If there’s a long gap in your eating schedule (say, breakfast at 10 am and dinner at 6 pm), watch what your blood sugar does in between. Rising levels suggest you need more basal insulin; falling levels suggest you need less.

Our goal is to protect your personal health information. Please keep your questions general and do not post personal medical information here. If you have a specific question, please email events@tcoyd.org.