The Patient:
Josh is a 36-year-old male who was diagnosed with diabetes at the age of 25. Many healthcare professionals would have automatically assumed Josh had type 2 diabetes because of his age, but Josh’s correct diagnosis was LADA – latent autoimmune diabetes in adults. LADA is essentially your run-of-the-mill type 1 diabetes that’s just diagnosed later in life. The more common age for someone to be diagnosed with type 1 is as a young child or teenager.
Adults with LADA have no real symptoms for a while, but eventually they may experience excessive thirst, frequent urination, and noticeable weight loss. Josh experienced all of these symptoms despite eating a healthy diet and exercising consistently. Josh doesn’t have any family history of diabetes (which is typical of many people with type 1) and he is not overweight. He does not have hypertension or abnormal cholesterol or triglyceride levels, which are classic for someone with type 2 diabetes.
Thankfully, Josh was diagnosed correctly right off the bat with the help of a T1D autoantibody test called GAD, and he was able to focus on managing type 1 from the get-go.
The Regimen:
Josh’s diabetes control is excellent. He uses a continuous glucose monitor and is on a regimen called MDI or multiple daily injections. He uses a long-acting basal insulin (Lantus) and a fast-acting insulin (Novolog) to cover his meals and correct for elevated glucose levels anytime. He chose this regimen because he is an avid CrossFit guy who does crazy things at the gym, and a pump would get in the way (or get ripped off by accident).
Josh’s CGM Download Data:
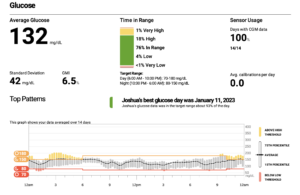
You can see he has a mean glucose of 132 mg/dL, an estimated A1c (or GMI) of 6.5%, a standard deviation of 42 mg/dL (the goal is less than 50), time in range (TIR) of 74% (the goal is above 70%), and time below range of 4% (the goal is 4% or below). His 24-hour glucose profile is fairly flat, with some lows between 1:00 a.m. and 2:00 a.m. In fact, Josh is doing just as well (or better) than other people with diabetes who are on an insulin pump therapy!
We Can Learn Many Things from Josh’s Case:
- You can get type 1 diabetes at any age, and it is not uncommon to be misdiagnosed when you are diagnosed later in life.
- It’s important for people with diabetes to have options for their diabetes management. Someone like Josh prefers being treated with a CGM device and MDI because it fits his lifestyle of being an avid CrossFit enthusiast.
- Josh’s glucose control is close to perfect on shots, but in my humble opinion, he could benefit from one of the second-generation basal insulins such as Toujeo or Tresiba, which would flatten out his basal profile and potentially avoid those lows in the early morning most likely caused by his bedtime Lantus dose. I would also recommend the use of an ultra-fast-acting insulin such as Afrezza to prevent any post-meal spikes, and to correct elevated glucose values as well.
The Takeaway:
If you were diagnosed with type 2 diabetes as an adult and you think you might have type 1, push for an autoantibody (GAD) test. Discuss treatment therapy options with your doctor to determine which type of regimen is right for you and your lifestyle. There’s more than one way to ace your diabetes management, and it’s never too late (or early) to start.

thank you for this information. How can I find information about when is the best time to start insulin for LADA.
I’m much older than Josh . . . DK if that matters. Sugar and A1C levels remain in barely pre-diabetes levels, but I recently tested positive for GAD (and have family and personal history). Is there some blood sugar level that triggers the need? Endo says there’s evidence that starting early could prevent/forestall ultimate insulin dependence, but I can’t find anything near conclusive.
thoughts?
Very simple answer…when your glucose levels start to elevate into the diabetic range and your A1c is 6.5, or creeping up.
Maura read up on how some patients have found they need less insulin on Ozempic or Manjouro. It is possible you still have C-peptides and can preserve your insulin production with another off label diagnosed drug or attempt to get Tzield. Being insulin dependent isn’t a terrible thing, but if you aren’t there yet I completely understand why you would give all your fight to preserve what your body does. Some have found success eating vegetarian diets, with large doses of Vitamin D and lots of exercise to maintain dependence from insulin shots. IT’s a commitment that many find too daunting and if you are nearly out of c-peptides it is likely too late.
have the same case as Josh. I was diagnosed with diabetes at the age of 25. After six months, my doctor suggested I start insulin. Now I’m 34, and I am wondering which test I could do to identify my type of diabetes.”
Hi Ammar,
You need to get the panel of insulin autoantibodies, including GAD because that’s the most important one. But I would get the whole panel.